hyponatremia in burn patients, check these out | Do burns cause hypernatremia or hyponatremia?
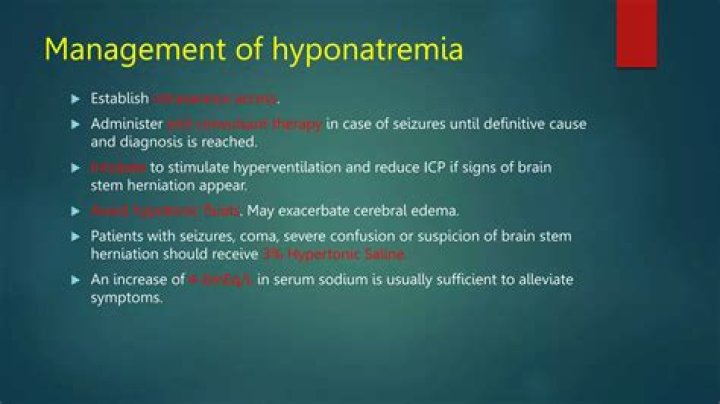
Low urinary sodium concentration is caused by severe burns, gastrointestinal losses, and acute water overload. Management includes instituting immediate treatment in patients with acute severe hyponatremia because of the risk of cerebral edema and hyponatremic encephalopathy.
Do burns cause hypernatremia or hyponatremia?
In critically ill burn patients, hypernatremia is a common condition and can occur in up to 11% of severely burned patients. The most common etiology underlying the development of hypernatremia is loss of total body water through insensible losses and sepsis [22, 23].
What electrolyte imbalances occur with burns?
Third-degree burns can sometimes lead to dehydration because they damage the entire thickness of the skin and affect nerve-endings. They leave the body more open to lose fluids. The layers of skin keep fluids inside the body. Fluid will often seep from the burned area, causing dehydration and electrolyte imbalance.
Do burns cause hypo or hyperkalemia?
Introduction: Classically, hyperkalemia has been regarded as a complication in patients with electrical burns. The etiology of hyperkalemia includes metabolic acidosis, destruction of red blood cells, rhabdomyolysis and the development of renal failure.
Why do burn patients have hyperkalemia?
Burns or other severe injuries. This occurs because your body, in response to severe burns or injuries releases extra potassium in your blood. Poorly controlled diabetes. When diabetes is not controlled, it has a direct effect on your kidneys which are responsible for balancing potassium in your body.
What happens to sodium in burn patients?
Abstract. Following burn injury, as after other forms of trauma, there is renal sodium and water retention with increased urinary potassium losses. The hyponatræmia in these cases results rarely from sodium deficit but usually from excess water retention and entry of sodium into the cells.
What causes fluid shift in burns?
Burns and Wounds
After a burn, fluid shifts from vascular to interstitial and intracellular spaces because of increased capillary pressure, increased capillary and venular permeability, decreased interstitial hydrostatic pressure, chemical inflammatory mediators, and increased interstitial protein retention.
How dehydration occurs in burns?
Dehydration. In severe or widespread burns, fluid is lost through the skin, and the person can become dehydrated. Dehydration can lead to life-threatening shock. A doctor will treat dehydration with intravenous (IV) fluids.
Which of the following fluid imbalances would result from severe burns?
Severe burn injury induce a capillary leak characterized by fluid dysregulation, electrolyte imbalance, loss of proteins and circulatory insufficiency [1], [4]. Fluid resuscitation within the first 24 hours after burn injury is commonly monitored by measuring urinary output, haematocrit and mean arterial pressure.
What is the resuscitation phase of burn injury?
In the hours immediately following a major burn injury, loss of capillary permeability allows intravascular fluid to flood into the extracellular space. During the emergent or resuscitative phase, efforts are directed at preventing or reversing burn shock using fluid replacement for- mulas.
Why is succinylcholine contraindicated in burn patients?
Succinylcholine is safe in the first 24 h after a burn—after this time, its use is contraindicated due to the risk of hyperkalaemia leading to cardiac arrest, thought to be due to release of potassium from extrajunctional acetylcholine receptors. This can persist up to 1 year post-burn.
What causes infection in burns?
Wounds can become infected if bacteria get into them. If your burn or scald has a blister that’s burst, it may become infected if it’s not kept clean. Seek medical attention for any burn that causes a blister.
What are 3 causes of hyperkalemia?
The leading causes of hyperkalemia are chronic kidney disease, uncontrolled diabetes, dehydration, an injury causing severe bleeding, consuming excessive dietary potassium, and some medications.
What are the clinical symptoms of hyperkalemia?
Hyperkalemia symptoms include:
Abdominal (belly) pain and diarrhea.Chest pain.Heart palpitations or arrhythmia (irregular, fast or fluttering heartbeat).Muscle weakness or numbness in limbs.Nausea and vomiting.
What are the ECG changes in hyperkalemia?
ECG changes have a sequential progression, which roughly correlate with the potassium level. Early changes of hyperkalemia include tall, peaked T waves with a narrow base, best seen in precordial leads ; shortened QT interval; and ST-segment depression.
Why do burn patients have hyperglycemia?
Burn patients are utilizing non-carbohydrate sources to generate glucose (gluconeogenesis) resulting in an increase in glucose production (glycogenolysis). These patients also have high insulin resistance, resulting in a poor response to insulin (Mecott, 2010).
What causes metabolic acidosis in burns?
The decreased cardiac output is due to loss of intravascular volume, direct myocardial depression, increased pulmonary and systemic vascular resistance (PVR and SVR, respectively), and hemoconcentration and can lead to metabolic acidosis and venous desaturation (↓SvO2).
Related Archive
harry potter wizards unite wand guide, latest free online harry potter movies, best HD videos you should watch in 2022 – 2023

harry potter villain test, latest free online harry potter movies, best HD videos you should watch in 2022 – 2023
harry potter uk edition books, latest free online harry potter movies, best HD videos you should watch in 2022 – 2023